Full Report
Welcome to your free report covering the diagnosis, management and treatment options, exercises and equipment that could help in rehabilitation. Scroll down to read more or use the sidebar icons to skip ahead.
Diagnosis
Oblique Strain
Your obliques are made up of two muscles and are part of an overall group called your abdominals. Your abdominals are a group of muscles on the front and side of your torso. There are four muscles which make up this group and they are the rectus abdominis, transverse abdominis, and the internal and external obliques. As a group they help offer stability to your trunk during movements, along with generate movement of the trunk forwards and sidewards. The rectus abdominis are on the front of your torso and are what people would call the 'six pack muscles'. They attach onto the front of the ribs and onto the front of the pelvis, and help with forward movement of the trunk. The transverse abdominis is the deepest abdominal muscle and wraps around your entire torso attaching onto the bottom ribs and the top of the pelvis, it's role is to offer stability to the trunk during movement. The internal and external obliques are situated on the side of your torso attaching to the ribs and pelvis, and their role is to help with sidewards and rotational movements of the torso along with adding stability to movements. These muscles generally work as a group, but certain movements can cause more load to be put on specific muscles. For example if you were carrying some shopping bags in your left hand, the obliques on your right side would be working to keep your torso upright.
These muscles attach onto the ribs or pelvis by a tendon. A tendons role is to attach muscle to bone, and then help transfer the energy produced by the muscle into movement. These tendons are very strong and adaptable to the load and activity that they are required to perform. However, if the load or demand they are put under is too high to what they can handle, they will become slightly damaged and cause pain, this is called a tendinopathy if it is over a period of time, however if it is a specific event this damage will be termed a strain.
The term 'strain' is used to describe a condition when small tears occur in muscles or tendons causing pain usually as a result of overexertion or overstretching from a specific event.
From the testing you performed you had no pain on hip flexor or adductor resisted testing, and there was no pain with hip flexor or adductor stretching. You also mentioned there was no change in the type or intensity of activities you performed, so we can presume this injury is from a specific event where perhaps you overstretched or overexerted yourself. You also didn't experience discomfort when you performed the plank exercise which leads us to believe your abdominal muscle group are not irritated. However it was painful when performing a side plank which suggests that the obliques may have suffered a strain of the muscles or tendons. On the front and inside of your hips there are lots of muscles crossing over and it can be difficult at times to pinpoint one specific muscle which is the cause of your pain, and it may be the case there are multiple muscles or tendons which may be strained. The obliques attach onto the front of the pelvis and it may be this area which has suffered the strain.
With this programme we have included exercises which will also address any issues which may be attributed to your symptoms from the other muscle groups around the hip. It is not uncommon for hip pain to be caused by an imbalance of muscles where one group has to work harder to compensate for weakness elsewhere. This episode however could just be down to some poor luck, that the action you performed put too much load or stretch on a muscle or tendon, or group of muscles, to what they can handle which resulted in a strain.
You also answered at the start that there is no pain with coughing or sneezing and no swelling present, which gives us confidence that there is no hernia present. If this changes during your recovery you should seek advice from your family doctor.
With a strain the important thing to know is that these heal well as long as during the muscles or tendons rebuilding phase the load put through them is reduced to an appropriate level. So for example, in the early stage you may need to reduce activities which put the abdominals under a high load, such as heavy lifting, sprinting or performing sit up type movements. A common misconception with a muscle or tendon strain is the desire to stretch out what feels like tightness. All this will do is pull apart an already damaged piece of soft tissue and disrupt the healing. You will want to stretch the muscle and tendon as normal later on during your rehab but not initially. Instead by progressively loading the affected area whilst it is healing will help with the rebuilding process, and make sure the strength of your muscles and tendons progress as you are healing.
Regardless of the underlying cause the initial treatment is the same, and the programme has been designed so that if there were any weakness which would have contributed to the injury, these will be addressed.
Management
Click each phase heading to see the progression of your management programme.
This phase is normally the first 24-72 hours after the event that has triggered your symptoms and its aim is to settle any swelling and pain whilst maintaining the range of motion and function you have. You may find the steps in this phase not applicable due to the level of movement and pain you have, or you may find only a number of points helpful. If you have no pain with daily activities and full range of movement of the hip, you could simply miss this step and start on Phase 2.

RICE
RICE stands for Rest, Ice, Compression and Elevation. These steps are helpful for when you have an injury in the acute phase to help reduce pain and also with the healing process. With an injury where the obliques are impacted it is generally impractical and not particularly beneficial to perform the elevation part of this treatment method.
Rest: You need to reduce the activity level you are performing and let your body have time to heal. The aim here is to pace your activities throughout the day and cut back on anything unnecessary or that particular increases your symptoms.
Ice: This can help reduce the pain you are experiencing and also reduce some of the swelling if you have any. Using some frozen peas wrapped in a damp cloth for 20 minutes will work well here and do this every hour or two. Do not apply the ice directly to your skin, make sure you have a barrier which is preferably damp, and keep an eye out for any ice burns onto the skin. If you notice this stop immediately.
What can be helpful here is having a specifically designed ice pack you can reuse over and over again. You still need to have that damp cloth as a barrier with these packs as well.
Compression: This relates to the use of the ice being compressed onto the hip region. This can be achieved by simply wrapping a cloth around your joint, but more bespoke equipment offers this ability which would be more comfortable and effective, such as a hip ice pack.
Medication
In the initial phase the use of over the counter medication may be an option. Medication such as paracetamol and ibuprofen may allow this acute phase to be more manageable. Please consult your family doctor if you have any concerns with this impacting your current medication, or if any medical history may be impacted by the option of including this medication.

Exercises
In this early phase there are no specific exercises you need to complete. Simply going for a slow walk and potentially adapting how you perform specific daily tasks which involve lifting will be helpful to allow your muscles some time to recover.
This would be roughly the first 2-4 weeks of your recovery.

Education
The aim here is to ensure the muscles surrounding your hips remain strong and we start to address any potential imbalances. There shouldn’t be any pain with these exercises so if you do experience this try to reduce the intensity or simply stop them until you have moved further along the healing pathway.
Muscles and tendons can take up to 12 weeks to repair and in some circumstances longer, depending on the severity and also the individuals specific activities they want to perform. During the early stages of recovery you need to be cautious not to overload your muscles and tendon and cause a spike in pain and also further irritation to the soft tissue. This may result in a backward step and delay in your recovery. Equally important is not loading the soft tissue enough. It is a balance to create and unfortunately you won’t get it right every time, however as long as you don’t keep getting it wrong, and each week you are loading the hip flexors more, then you are heading in the right direction.
The abdominals are made up of four muscles, the rectus abdominis, transverse abdominis, and the internal and external obliques. As we have mentioned at the start these muscles are involved in giving the torso stability. Generally with any lifting or exercise in general, these muscles are activated to some extent. So during your daily activities they will be working, and during the exercises in this phase even though they aren’t being isolated, they are still getting loaded.
Tendons and muscles love load, but it needs to be the right level for what they can tolerate for that period of time. You want to reintroduce load to the tendon and muscles, and progressively load it so it can tolerate more. This ability to tolerate more load will mean you can perform more tasks day-to-day and eventually return to your sporting or daily activity of choice.
You will hopefully start to notice that general daily activities become easier as you reduce the load which was aggravating your symptoms and your tendons begin their healing process. Try and avoid the temptation in the start to repeatedly poke and massage the tendons as this could potentially irritate it further.
Exercises
A benefit of performing exercises which are hopefully relatively easy, is that it allows some time for any irritation in your obliques to settle whilst it still gets some low level load through it. The evidence has shown that after a short period of rest, you want to load a tendon or muscle at an appropriate level to help with the healing.
The aim of these exercises is to introduce some basic strength work to the surrounding muscles in the hip and legs without aggravating the obliques. Remember to start off easy and only increase the intensity each week once the symptoms have settled.
A good marker of when to progress from this phase is when you no longer get any pain with daily activities.
You may find it helpful to perform the exercises in Phase 1 as a warm up before attempting these.
| Exercise | Frequency | |
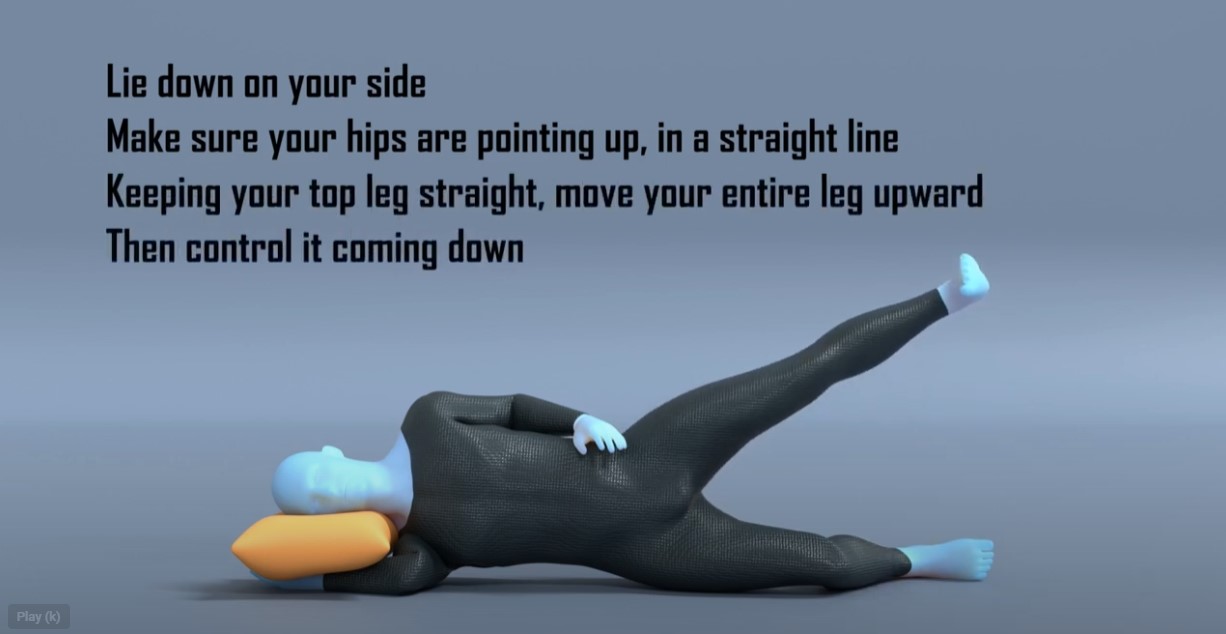
| Side Lying Hip Abduction | 30 - 60 secs x 4 sets | 2 x daily |
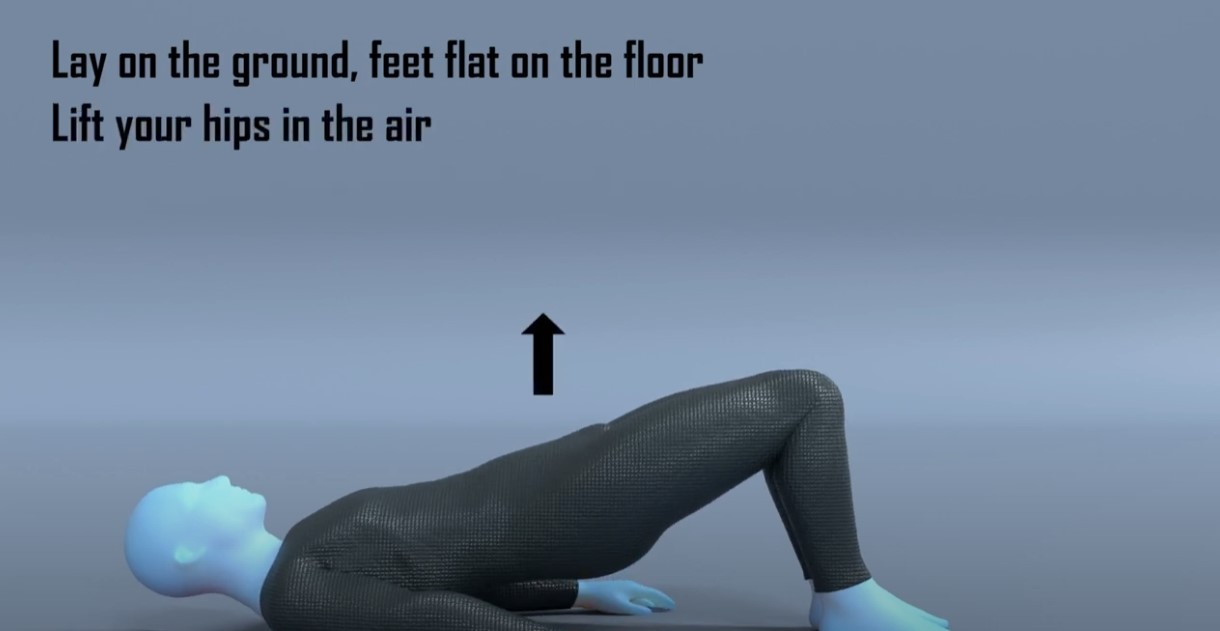
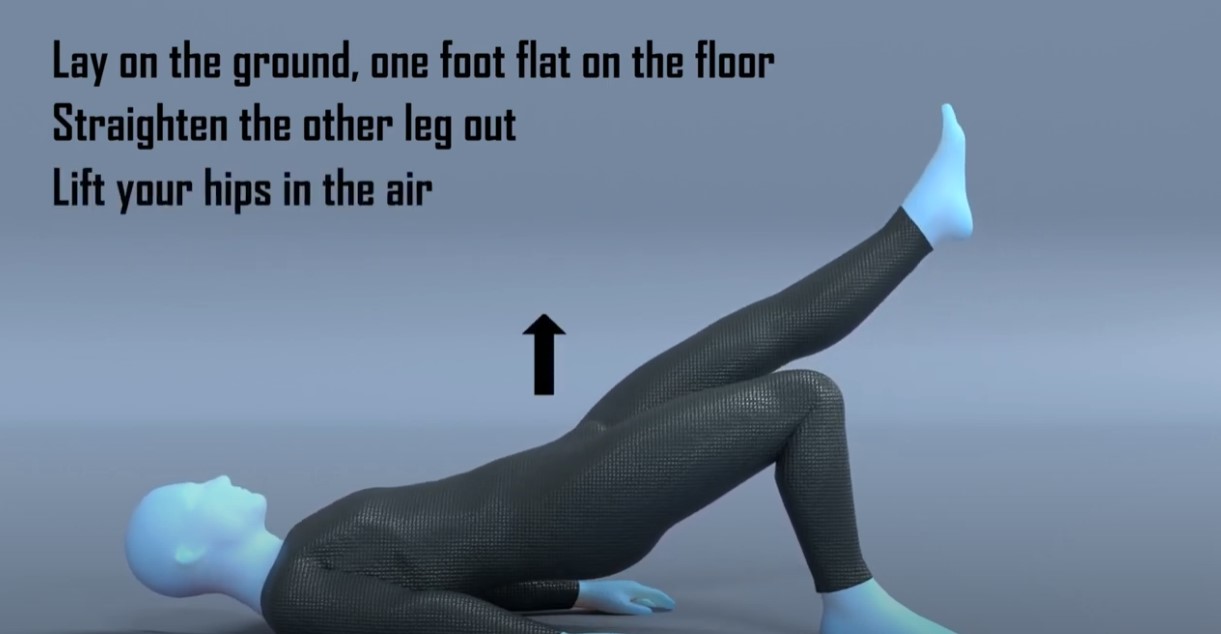
| Double Leg Hip Bridge | 12 - 15 reps x 4 sets | 2 x daily |
| Kneeling or Full plank | 12 - 15 reps x 4 sets | 2 x daily |
Some things to consider with the exercises:
- The exercises in this phase are to reintroduce some progressive load work onto the muscles surrounding your hips. We have purposely put the isometric hip flexor exercise last as this exercise may be the hardest so having a few exercises warm up before may help to complete this exercise.
- The first and second exercise is aiming to ensure our glute muscles are strong and help us with general hip control. If you find this exercise too easy you can put on some ankle weights or use a resistance band to make it more challenging.
- The final exercise may be the hardest but as you were pain free on testing you should hopefully be able to manage this without discomfort. There are many adaptations you can try to vary the intensity depending on your fitness and symptom level. Start with performing this exercise on the floor on your knees. If you find this too painful you can make it easier by performing it against a table or wall. This will reduce the angle and ultimately the load put through the abdominals. If however you can perform this on your knees for 60 seconds you could try and perform the full plank where your body is completely straight. You would need to reduce the duration back to 30 seconds as this exercise is now harder, and then progressively build back up.
- You may find it helpful to do these exercises in a circuit type fashion, where you do exercise 1 for 1 set, followed by exercise 2 for 1 set, then exercise 3 for 1 set. Make sure you have a rest after exercise 3, of at least 1 minute, before restarting at exercise 1.
Medication
You should expect to see the usage of medication reduced as you move through this phase. If you require medication to get you through the exercises, or immediately afterwards, perhaps you need to reduce the reps or duration of some of the exercises so that it becomes a little easier.
Massage
Given the location of your symptoms and the fact the obliques are involved, it is unlikely that massage will offer much benefit to you. Massage over your obliques will be discomforting at the best of time due to the organs underneath this muscle group, and any light pressure techniques would not be particularly effective.

Strapping
Kinesiology strapping is very popular for many musculoskeletal injuries. The idea is that the tape helps support the muscles and tendons at the point of pain, and therefore causes less pain when doing exercises or general daily activities. The evidence for kinesiology strapping is mixed, and because of that some people find it’s really helpful whereas others find it doesn’t offer them much at all.
If you feel you are struggling to progress, or you feel your rehab is a little stagnant, or that general daily activities are still irritable, then it may be helpful to try this.
You can leave the tape on for up to 5-7 days but at any point if it feels hot and itchy take it off straight away. Have a day's rest of no tape before reapplying, and ideally test with a small strip before applying a big amount to you.
This video shows a general strapping method which you may find helpful, but as your symptoms are more over the front of your hips it may not add much relief.
It’s likely that used alongside some of the other treatment methods it may offer some relief, but realistically on its own will not help completely alleviate your pain.
Symptoms
During this phase you should start noticing more times in the day when you are pain free, however it is not uncommon for there to be sharp spikes in pain if you are doing a specific activity especially heavy lifting. This will improve and the activities which cause irritation should become less. If you continue to perform activities which consistently aggravate the obliques, it will continue to cause you pain and perhaps be affecting the end stage of healing. You need to alter the activities in some manner that are causing irritation until you have moved further along in your healing, and increased the strength in your hip flexors.
If you are struggling to wean off medication or perform the exercises in this phase it may be helpful to be reviewed by a medical professional to ensure you are on the right path. If they confirm it is a strain then you can continue on the phases in this rehab programme.
In this phase we are looking at between 4 to 12 weeks following the injury or start of your symptoms.
Education
Similar to Phase 2 the timelines here are merely a guideline and may vary. You may find that you are able to start this phase before 4 weeks if the symptoms have settled and you aren’t challenged by the exercises.
The aim of Phase 3 is to increase the intensity of the rehab exercises, specifically the oblique loading exercises. You should now be looking at returning to full daily activities and depending on the severity of the strain and your chosen hobbies, a return to sport also.
You should at this stage be able to perform the exercises from Phase 2 with ease, especially the isometric hip flexion, and not reliant on any pain medication to perform daily activities.
For the vast majority it may be the case that we need to improve the strength of our obliques for some very specific day-to-day activities related to a hobby or our work. Others may have a specific long term goal in mind, such as returning to sport or another lower limb activity.
Exercises
The focus on Phase 3 is to move onto loading of the obliques and ensuring the general leg muscles remain strong, which will help ensure you have the capacity throughout to perform day-to-day movement.
If you remember the principle of muscle strain rehabilitation at the start of this programme, you want to progressively load up the hip flexors slowly over time.
| Exercise | Frequency | |
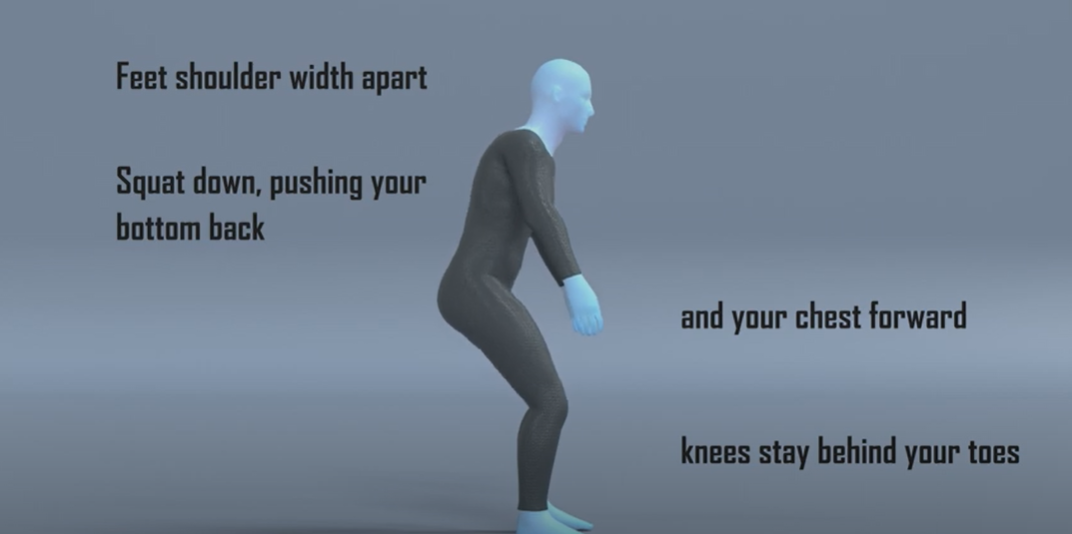
| Sit to stand or Squats | 10-15 reps x 4 sets | 2 x daily |
| Hip Flexion in Standing | 30 - 60 secs x 4 sets | 2 x daily |
| Kneeling or Full Side Plank | 30 - 60 secs x 4 sets | 2 x daily |
Some things to consider with the exercises:
- You may find performing the exercises from Phase 2 acts a nice warm up before attempting these exercises which are slightly harder.
- The sit to stand exercise is easier than the squat exercise. If you struggle with the sit to stand exercise, raise the height from which you perform this movement from, this will make it easier to perform. If your balance is your limiting factor here, you can gently hold onto something to give you some support. Your aim should be to have equal weight bearing on both feet, but it may be the case you need to progress on to this. If you are struggling performing the squat then regress to the sit to stand exercise. If you are able to perform the squat and it eventually gets too easy, you can progress this and hold some weight during the movement.
- The second exercise is loading the hip flexors and with this exercise you will also be bracing the abdominals to provide stability. Start initially just performing the movement in a slow and controlled manner. Once you can perform this for 60 seconds and 4 sets you can then start to increase the resistance or load of the movement. This can be achieved by putting on some ankle weights or using a resistance band wrapped around your ankle. When you add this resistance you may need to reduce the duration of each set initially and then build back up. If you do not have access to either ankle weights or a resistance band, you can simply keep your leg straight when you perform the movement and this will increase the demand of this exercise as the lever, your leg, will be longer.
- The final exercise is introducing the exercise which was initially painful in the testing. Start with the easier option of performing this on your knees for 30 seconds and progress once you are confident this is pain free. As with the front plank there are adaptations you can try to vary the intensity. If you find the exercise on the floor on your knees too difficult again try performing it against a table or wall. This will reduce the angle and ultimately the load put through the obliques. If however you can perform this on your knees for 60 seconds you could try and perform the full side plank where your body is completely straight. You would need to reduce the duration back to 30 seconds as this exercise is now harder, and then progressively build back up.
- You may find it helpful to do these exercises in a circuit type fashion, where you do exercise 1 for 1 set, followed by exercise 2 for 1 set, then exercise 3 for 1 set, and then restarting after a break.
The final phase may not be necessary for everyone, however if after completing phase 3 you are finding you are still not able to complete your activities or sport of choice pain free then it may be best to continue, especially if you need to hop or run.
If you have a desire to return to running or sport then you should continue with this phase.
Here we focus on performing exercises that are more dynamic and to mimic the demands of running, along with a bias onto the single leg. As we introduce impact work into the rehab programme you need to be conservative in these sessions and build up slowly. For the first week performing these exercises follow the rule that you want to leave each session wanting to do more. You do not want to finish the session and be in pain thinking that you have ‘now worked hard enough’. Starting impact work is a big step and generally what most people find the hardest. You want to be patient and not rush things, undoing all of the good work you have done up until this point.
A simple test if you have access to a leg press machine in a gym, is to see what your 1 rep max leg press is and compare it to your other leg. If you don’t normally use this piece of equipment some guidance from a Physical Trainer in the gym would be advised. What you are aiming to see is that your injured leg should be at 90% strength of your non-injured leg. If your injured leg is much below this number it may not have the strength to cope with the demands of running. Another way to test without a specialist kit is doing a single leg sit to stand test, where you count how many single leg sit to stands you can do on the injured side and compare it to the non-injured side. Similarly you want to be at roughly the same amount of reps for each side. Now these two tests are slightly different in that one will test max strength and the other more muscular endurance, but both will offer some insight depending on your access to equipment.
The second test you want to perform is the single leg hip bridge exercise. On the unaffected side initially perform this exercise for 20 reps and then repeat it on the other side. Was there a difference in fatigue or pain? If so it gives a good indication on what you need to work on. If there was no difference, repeat the test but increase the rep range to 30. You ideally want to be at 90% of effort needed to match the reps or 90% of the reps completed before moving onto any return to running or sport.
The exercises in this phase can help address any loss in single leg strength and will also help improve your single leg control, which will be crucial for any return to running or sport.
In this phase we are just continuing the process of increasing the progressive load onto the hip flexors. By this point you should be able to complete the exercises in phase 3 with good form and no increase in pain.
Exercises
| Exercise | Frequency | |
| Single leg sit to stand | 8-12 reps x 4 sets | 1 x daily |
| Walking Lunges | 12-15 reps x 4 sets | 1 x daily |
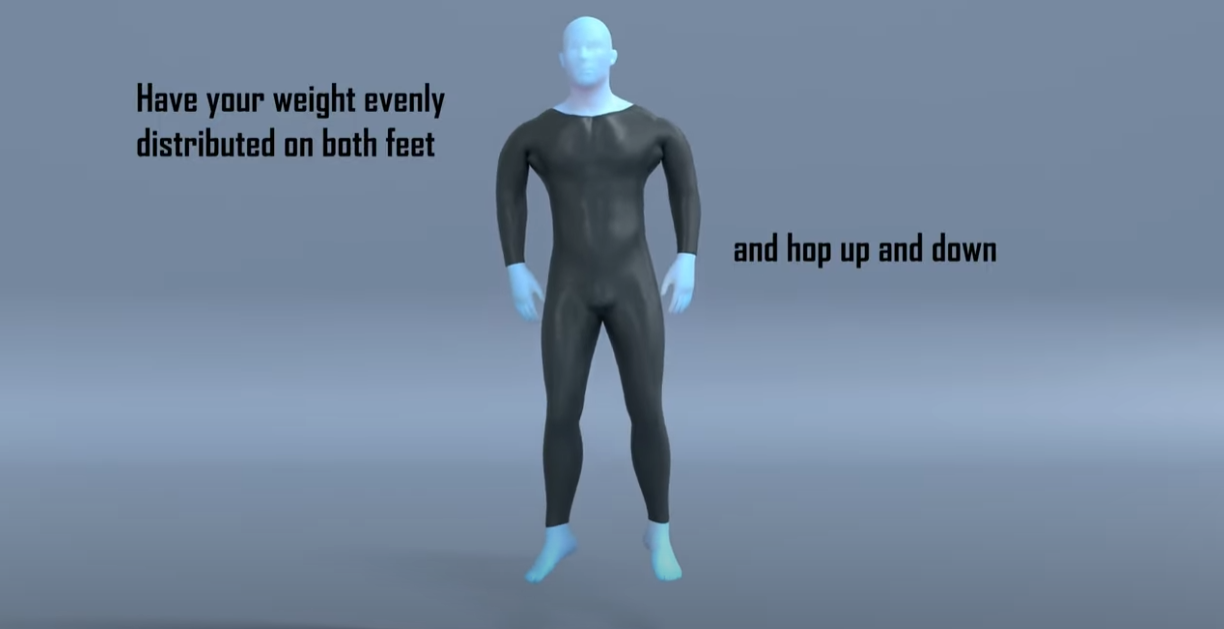
| Side to Side hopping | 30-60 seconds x 4 sets | 1 x daily |
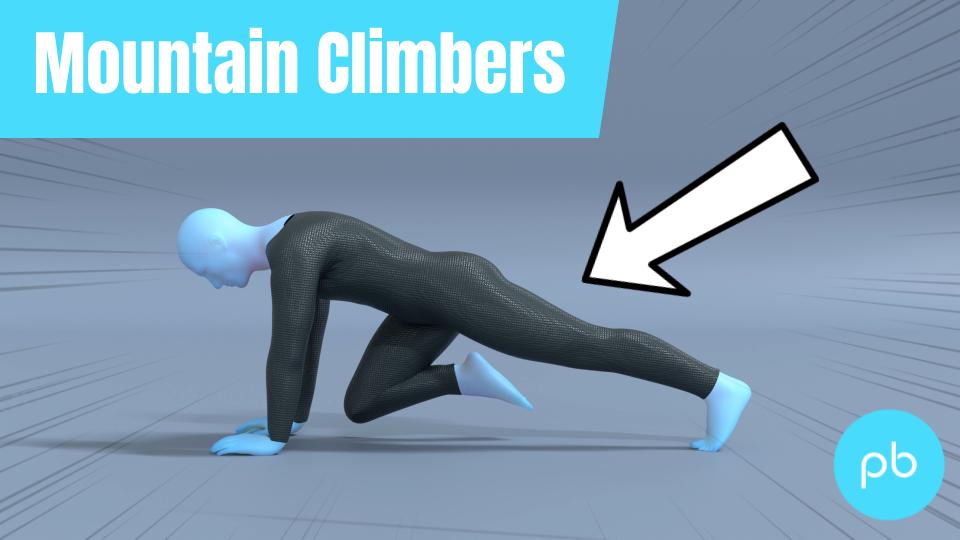
| Mountain Climbers | 30 - 60 secs x 4 sets | 2 x daily |
Some things to consider with the exercises:
- Performing the exercises in Phase 3 for one to two rounds may act as a good warm up for these exercises.
- If you struggle with the single leg sit to stand, raise the height from which you perform this movement from, this will make it easier to perform. If your balance is your limiting factor here, you can gently hold onto something to give you some support.
- For exercise 3 there may not be a necessity to perform this movement, and you may not have done any hopping movement for many years. If this is the case you can ignore this exercise and instead focus on the other exercises.
- The final exercise is similar to the plank exercise in the previous phase but adding some movement to make things harder. Start off by moving your legs slowly and as you become stronger and more confident you can increase it. This movement will also mimic the action and control needed for running.
- You may find it helpful to do these exercises in a circuit type fashion, where you do exercise 1 for 1 set, have a rest for 1 minute, followed by exercise 2 for 1 set, another rest for 1 minute followed by exercise 3, rest again before completing exercise 4, then a final minutes rest before then restarting.
Return to Sport or Activity
As a general rule, try and aim for two pain-free sessions at a reduced duration or intensity before increasing.
For example, if you normally play 60 minutes of tennis, aim to play for 30 minutes in a non-competitive environment for two non-consecutive days.
Having a day's rest between sessions allows you to have appropriate rest and for your body to repair and become stronger.
Once you have found a duration or intensity you can tolerate with no flare up, aim to increase the next session by 10%. This can seem like a slow and conservative process however the research has shown this is the optimum level of increase to avoid an overuse injury. Increasing duration or intensity by more than 10% significantly increases your chance of injury. As you will have been away from your sport for a number of months, you will have lost some of your fitness conditioning in this time and will need to build this up slowly.
Over time you will be able to slowly return to your pre-injury level of activity without regressing back to any acute flare-up.
Pacing
At this stage you should find you can do more day-to-day activities pain free. The temptation here is to go a bit overboard. A nice reminder to pace activities so that you don’t over do it, and that you spread these activities out as much as possible throughout the day.