![]()
This phase is normally the first 24-72 hours after the injury and the aim is to settle any swelling and pain you have. You will be able to apply the majority of the steps in this Phase alongside organising any x-ray or clinician assessment.

X-Ray and Assessment
Your first line of treatment should be to organise an x-ray to determine if there is any fracture of the patella. Please follow any specific instructions from the clinical team on timelines and activity limitations depending on the result of your x-ray.
If the x-ray showed no fracture it may be helpful for a physiotherapist or family doctor to assess your PCL. There is a simple test they can perform which will indicate to them if further investigation, such as an MRI, is needed.
RICE
RICE stands for Rest, Ice, Compression and Elevation. These steps are helpful for when you have an injury in the acute phase to help reduce pain and also with the healing process.
Rest: You need to reduce the activity level you are performing and let your body have time to heal. The aim here is to pace your activities throughout the day and cut back on anything unnecessary or that particular increases your symptoms. You may also find crutches at this stage are needed if the pain levels are too high for you to walk unaided.
Ice: This can help reduce the pain you are experiencing and also reduce some of the swelling. Using some frozen peas wrapped in a damp cloth for 20 minutes will work well here and do this every couple of hours if possible. Do not apply the ice directly to your skin, make sure you have a barrier which is preferably damp, and keep an eye out for any ice burns onto the skin. If you notice this stop immediately.
What can be helpful here is having a specifically designed ice pack you can reuse over and over again. You may still need to have that damp cloth as a barrier with these packs as well.
Compression: This relates to the use of the ice being compressed onto the knee. This can be achieved by simply wrapping a cloth around your joint, but more bespoke equipment offers this ability which would be more comfortable and effective, such as a knee ice pack. You may find that this aspect does not offer relief as the compression is discomforting, and in which case you should stop. Be conscious of any change in sensation in your foot or toes as a sign that this isn’t appropriate for you at this time.
Elevation: Having your foot rested on an object which is raised above your hips, whilst you are laying down, will reduce the amount of swelling in the area. This may help reduce some of the symptoms you are experiencing. Aim here for a similar time frame as applying ice and go for up to 20 minutes. Do not compress and elevate at the same time, as the volume of fluid returning towards your heart may put too much pressure on it.
Medication
In the initial phase the use of over the counter medication may be an option. Medications such as paracetamol may allow this acute phase to be more manageable. Some consideration in the use of ibuprofen at this stage should be given due to the evidence it may impact bone healing. Please consult your family doctor if you have any concerns with this impacting your current medication, or if any medical history may be impacted by the option of including this medication.

Support
If a fracture is seen on x-ray you may be required to use what is called a ‘cricket splint’ knee brace. This is a brace which limits the movement of the knee and gives it an opportunity for it to heal properly. You need to make sure the brace you are using is long enough to limit knee movement thanks to its solid structure, as a knee brace which is too short won’t give enough support.
Unfortunately knee brace options for PCL injuries, and to an extent ligament injuries in general, is a little less straightforward.
There are specific braces designed to offer support for PCL and ACL injuries which, thanks to their design, limit the movement and force on the knee in very unique ways. These braces are fairly expensive and would require a fitting by a specialist, versus trying to pick one off the shelf to do it yourself. However they certainly have their place and would be an option to explore if you needed one.
There are general hinged knee braces which offer an element of support for the knee which may be suitable in the interim either before committing to a more expensive brace, or perhaps if you have such a low level injury this option is suitable just to help support the knee whilst your injury settles.
Be cautious with any brace which is cheap and without proper support as this will unlikely offer any benefit. Something like a general neoprene knee brace is probably not going to be particularly helpful for you right now.

Exercises
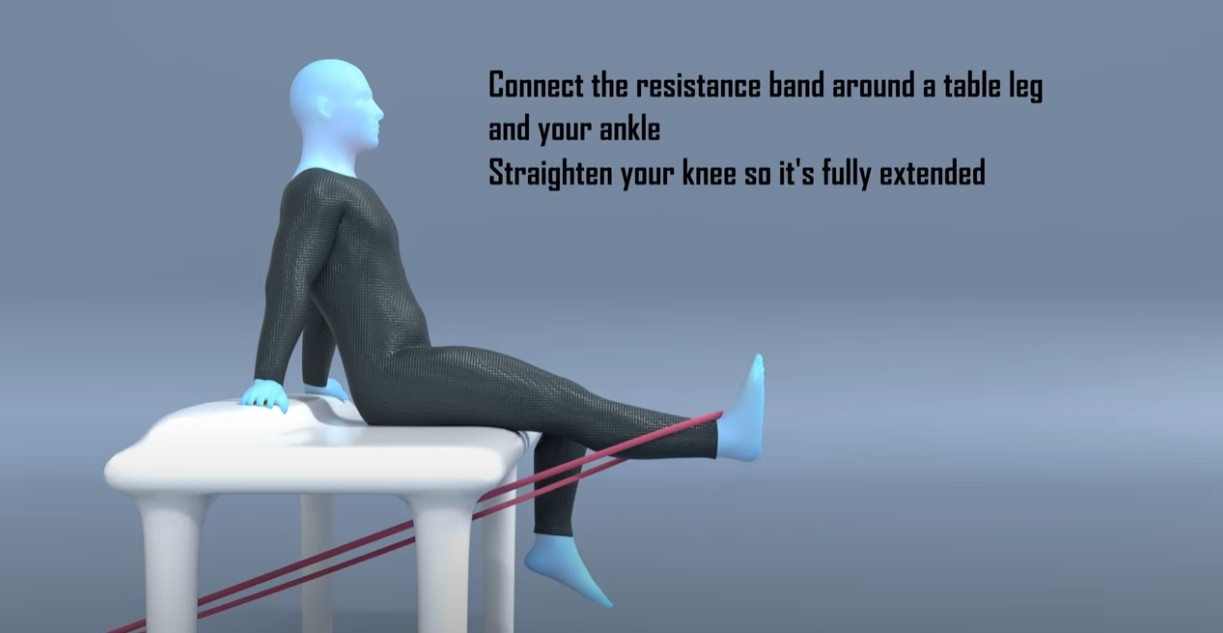
In this acute phase you should follow the guidance from the clinical team following the results of your x-ray, and potentially any MRI scan that you had. The exercises here can be started whilst you are waiting to get the x-ray and any other appointments organised, where the aim is to help with blood circulation to the area and to maintain the engagement of the quadricep muscles. With this type of injury and the potential level of pain you may find you are using your leg a lot less, which will result in your quadricep muscles not being activated. It’s really important we keep these muscles engaged and active as much as possible.
The main focus of these two simple exercises in this acute phase is to encourage blood flow to the area and engagement of the quadricep muscles.
| Exercise | Frequency | |
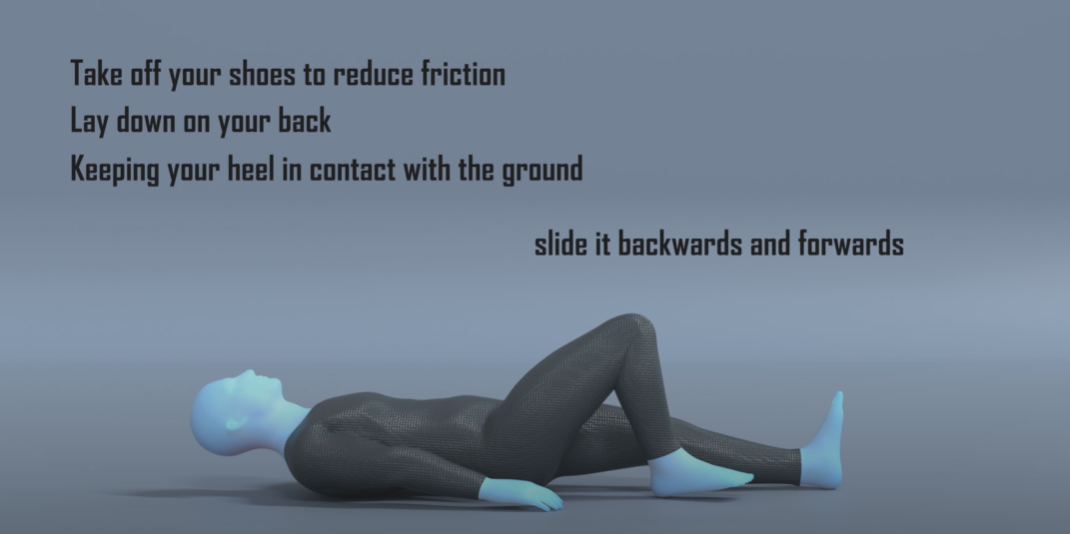
| Ankle Pumps | 30-60 seconds x 2 sets | 3 x daily |
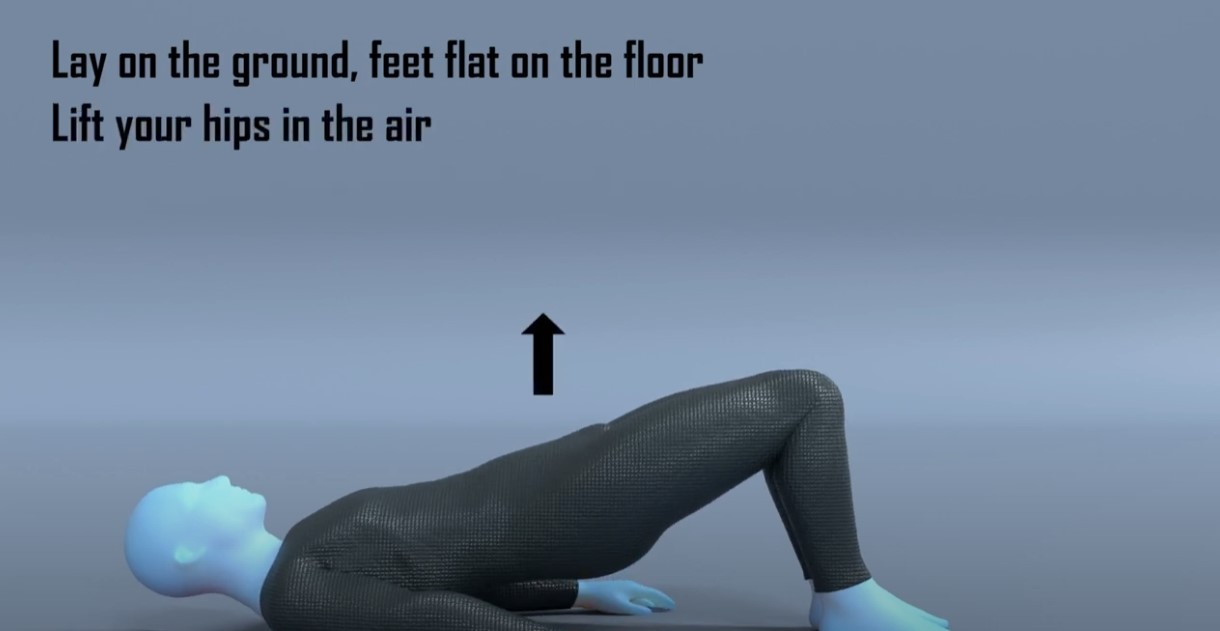
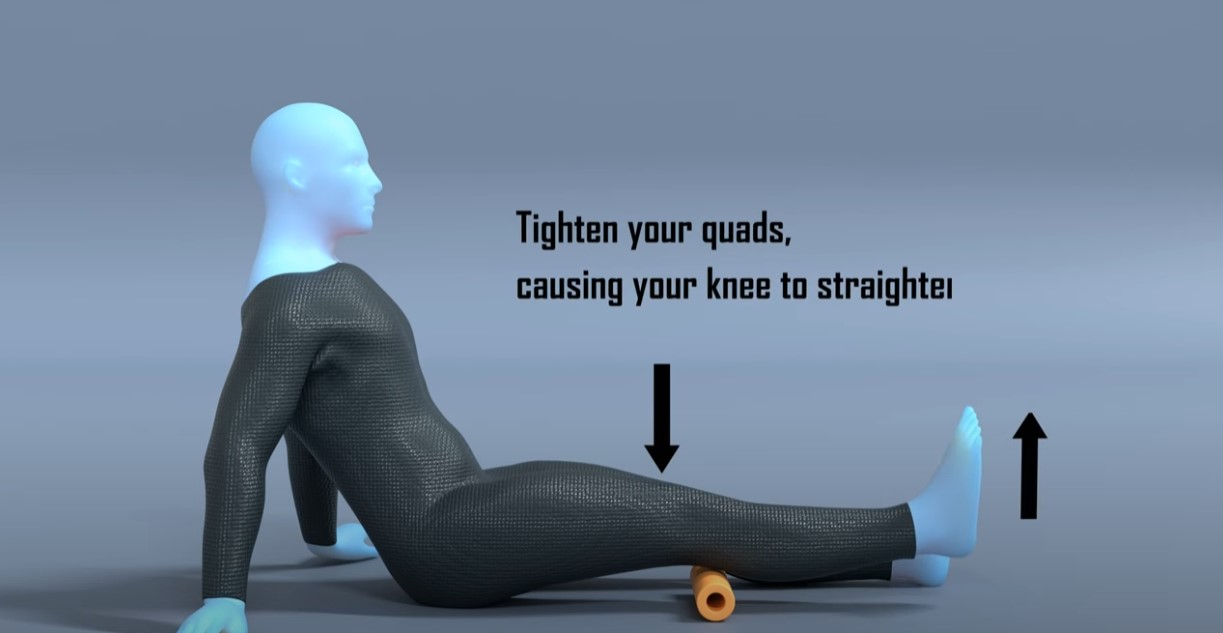
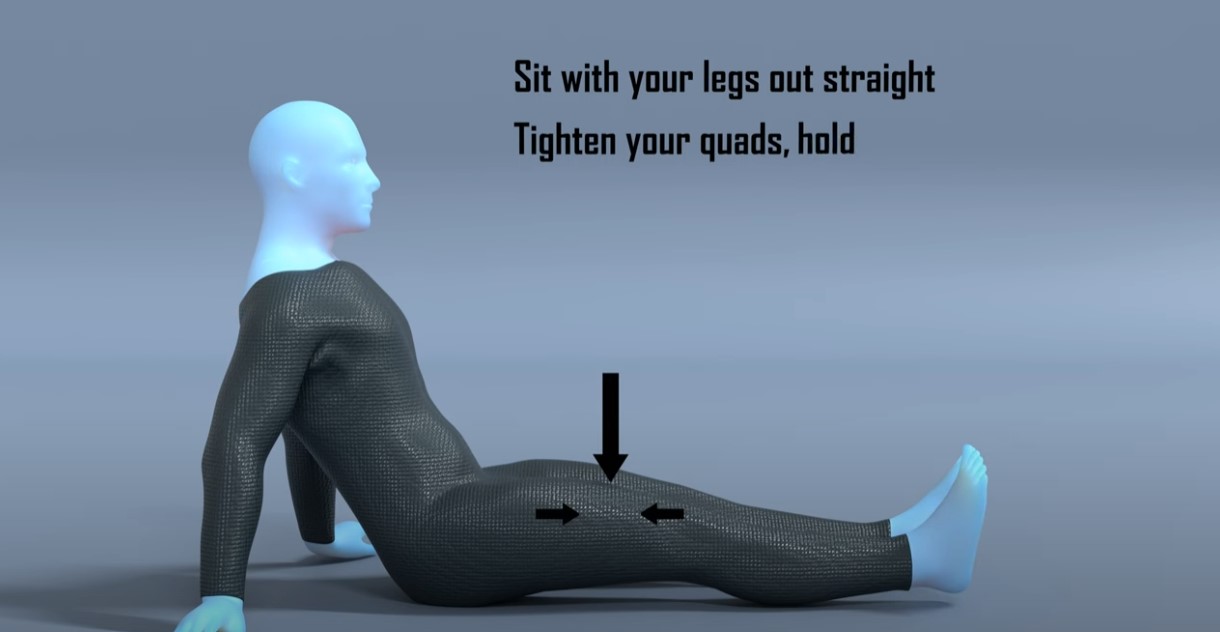
| Static Quads | 12-15 reps x 2 sets | 3 x daily |
Some things to consider with the exercises:
- The duration, sets and frequency you perform these is not set in stone, the important point to remember is to do these little and often throughout the day. This is better than doing them for one big chunk as doing them frequently for a shorter period will mean that the benefits are felt for longer throughout the day.
- Neither exercise should be painful but you may get some discomfort on the static quads exercise so either reduce the intensity you are performing this at, or stop it until your symptoms settle further.